We have received a number of questions from people asking about CDS and MMS1. In our communications it is evident that there exists a lot of confusion around this subject. Jim wrote in his MMS Health Recovery Guidebook, in Appendix A (page 307) his personal thoughts on MMS1, CDS and CDH. (Excerpts of this chapter are included at the end of this article).
Jim addressed this subject over the years, and since what he wrote in the MMS Health Recovery Guidebook, mainly during the “pandemic” era 2020—2023, Jim addressed this subject further, both in his writings which until now have not been published, as well as in personal conversations with various people, and in email correspondence. Below is a compilation of Jim’s stance on this subject, but first, we have listed points on the difference between MMS1 and CDS. It is our hope that this will help to clarify any questions, you, the reader, might have on this vast subject, and more importantly, in hopes that it may be of help to you, or your loved ones in obtaining optimum health.
Good fortune to all of you,
Team Jim Humble (March 10, 2026)
MMS1 Pros
- Tried and proven for many more years.
- Easy to mix up—put drops in glass, count to 30, add water, bottoms up.
- Not as finicky or volatile as CDS.
- Does not require refrigeration.
- If using citric acid crystals for activator it is easier to transport dry ingredients (SC [sodium chlorite] powder and CAC [citric acid crystals]), which is an advantage in certain situations and in many parts of the world.
- Goes deeper into the body, reaches the intestines and can go even deeper into the tissues. (*Further explanation on this below).
- If one comes to a “plateau” with CDS, (in other words comes to a standstill where no progress is being made) going to MMS1 can often bring results.
MMS1 Cons
CDS Pros
- Has a milder taste.
- Is good for external use, for all kinds of skin conditions.
- Very good for dental issues.
- Pure CDS is useful for injecting (CDI) with proper supervision, a plus for some conditions.
CDS Cons
- In the case of serious life-threatening conditions, it may necessitate the need to up the dose, however, CDS in large doses has a tendency to burn the throat.
- When necessary to take stronger doses of CDS some people do have nausea, diarrhea and/or headaches, in other words a herxheimer reaction or what is known as a “healing crisis”. This is often par for the course in the detoxification process and is not necessarily magically eliminated with CDS. Every case is different and many factors weigh in to this equation.
- Purchasing CDS online can be questionable, extensive study has shown many suppliers sell inferior quality product, much weaker than 3000ppm. (*See article below). For these reasons it is encouraged to educate yourself, learn to make it yourself and be diligent to follow instructions closely.
- CDS gasses out easily therefore strict diligence must be observed in handling it. Every time you open a CDS bottle, some of the CD gas escapes. So every use from the bottle is weaker than the previous one. This varies by temperature, how long the bottle is open and even the material of the bottle. The amount of air left in the bottle also can affect the strength as does UV light if the bottle is left out. You must handle it carefully and properly. Learn proper handling and storage guidelines.
- Requires refrigeration.
- Not always practical if on the move, traveling, etc.
- CDS does not reach the intestines. Watch this video where Andreas Kalcker explains this:
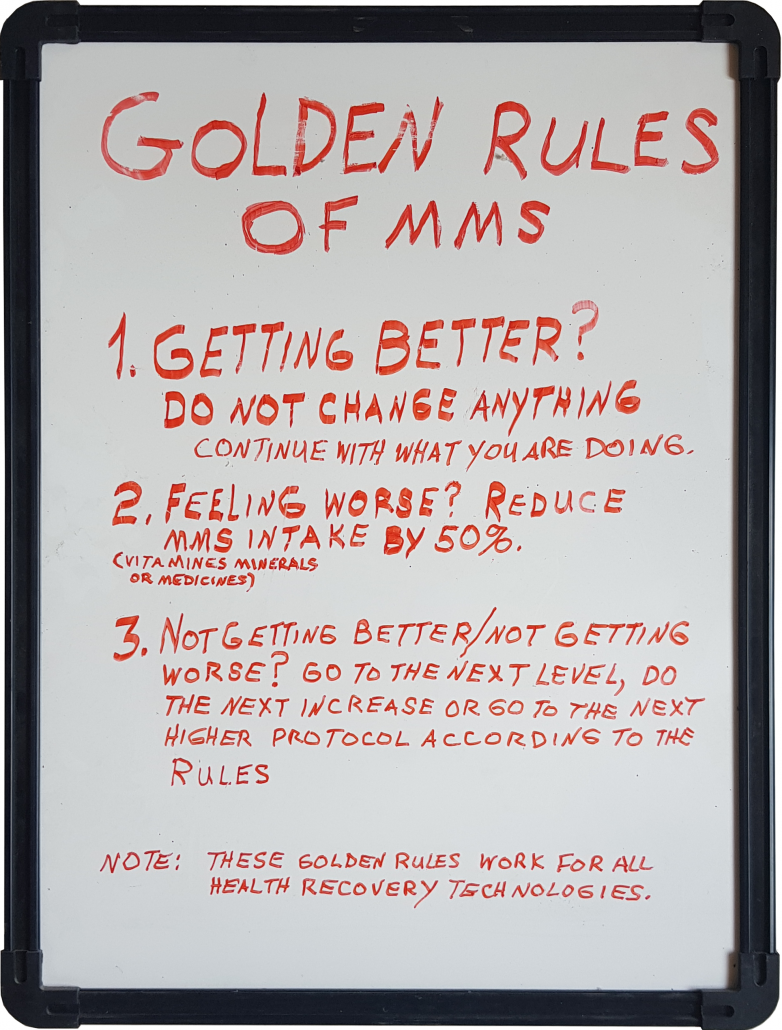
Note: At the end of this short video clip from Andreas, he mentions “overdoing” can cause an imbalance which can result in diarrhea or dehydration. The key here is to not over dose, go low and slow to start, be aware of these signs and pull back if needed—follow the Three Golden Rules of MMS.
- Some tout the fact that CDS is pH neutral. On it’s own it is, It is a neutral gas but when it comes in contact with water there is a reaction and it’s pH drops to acidic based on the type of water used. (*See more on this below from Dr. Martin Ramirez, COMUSAV)
MMS1 and CDS –Know the difference! And yes, they are different. Two forms of chlorine dioxide, but NOT entirely the same. Cousins but not identical twins.
It is difficult to compare CDS and MMS1, as far as the amount of chlorine dioxide (CLO2) that each can provide to a human body.
The reason they can’t be accurately compared is because MMS1 can continue releasing more CLO2 in stomach acid and sometimes beyond, but CDS cannot.
A 3-drop dose of MMS1 can contain up to 24mg of CLO2. A CDS dose of only 1ml = 3mg of CLO2. That is a big difference.
Let’s assume that 80% of sodium chlorite solution in a 3-drop dose of MMS1 gets activated. That would be about 19mg of CLO2. Still a big difference compared to 3mg from 1ml of CDS.
In this case you would need to ingest about 6ml of 3000ppm CDS hourly. That would likely bother your throat because CDS is 100% activated when made.
MMS1 is only 10% pre-activated at 30 seconds. More CLO2 can be released in stomach acid, depending on how much stomach acid is available, and this varies from person to person, and it varies throughout the day in the same person. In addition, beyond stomach acid, as MMS1 (which contains residual sodium chlorite) travels beyond the stomach and deeper into the tissues of the body, if it hits a pathogen which is normally acidic it can also further activate at that point, and release more chlorine dioxide, which can destroy the pathogen.
This is why, and as Jim taught, you cannot really compare CDS and MMS1 dosing. His personal conclusion on this was “While some people believe the advantage to CDS is that it does not contain unactivated sodium chlorite, I have a different opinion. I believe just the opposite.”
(*See full explanation on this below, taken from Appendix A from the MMS Health Recovery Guidebook).
Compilation of Comments from Jim Humble regarding MMS1 and CDS:
“Regarding MMS1 and CDS, I’ve already said this, but I’ll say it again—you can’t compare the two. Both are good, both work, both have a place, AND most importantly, in my opinion, one does not cancel out or replace the other. I have been hearing that some say MMS1 is old hat, or inferior—my answer to that is that is ridiculous. The real fact of the matter is it must be determined what to use in each case, according to the condition of the person.
There are usually many factors at play, and many times you have to dig deep, each case is different. People are bio-individual, so you have to find what is needed for each person, according to their condition. You need to be careful here, because if you try to put one down in favor of the other [say one is out and only use this now] it is my opinion, you are doing a huge dis-service to mankind you could be causing a significant detriment to people.
CDS has many great uses, and so does MMS1. Be careful not to favor one over the other, the question is to know when to use which one. There are many things to consider, first of all what the health condition of the person is, MMS1 and CDS work similarly, but they work differently as well. You have to also consider circumstances and conditions, availability and so on.
Just think, what if someone is very sick and they have neither the resources, nor the strength to make up their own CDS, and for whatever reason they can’t buy it online, that is not out of the question now-a-days when many people are worried about having enough toilet paper. But they have two bottles sitting in the cupboard, (bottle A and bottle B to make up MMS1) and hopefully they can muster up the strength or find someone to help them drop a few drops of each bottle into a glass and count 30 seconds, add water and drink it down. It could save a life, or eliminate a lot of pain! But if they have been taught one is “out now” they might not even try. That is not good!
You gotta be practical here—you can’t second guess everything, but give ‘em as many possibilities as you can to get well. What I am saying is you gotta look at all sides, first, the conditions of the body and determine which is best to take. Then you need to see what is “doable” for the person or persons to do in every situation, including what supplies do they have on hand, or what are they able to get and so on.
CDS has done great things, but that does not negate the fact that hundreds and hundreds of people have come to standstill when taking CDS and when switching to MMS1, they then recovered their health. We know CDS does not reach the intestines, MMS1 can go deeper into the tissues (see Appendix A from MMS Health Recovery Guidebook, excerpts of this are below), that has to be considered. CDS on the other hand is milder in some cases on the stomach and this may be an advantage to some individuals—again, it depends on what is going on in each individual body, it is not one size fits all. CDS can sometimes be injected if needed so that is a plus there. (Injections should always be performed by an authorized health professional). For goodness sake, this should not be a competition. All forms of chlorine dioxide work, and one needs to determine which form is right to use for their condition.
When I was out in the jungle, I contracted malaria myself and I was sicker than a dog. I somehow managed to get into town and I got tested. I wanted to document it, so I went to the hospital for the test. I was positive for malaria. I then took my water purification drops, and I was well in less than 4 hours. I went back and got retested and I was malaria free. So what did I do? I walked out of that clinic, stood on sidewalk and said to myself, I have to take this to the world. And that is exactly what I did. I didn’t patent it, I kept it grassroots for a long, long time, and it went around the world.
Now we have discovered new ways, new variations, we have MMS1, then came CDS and even CDH. All various forms of chlorine dioxide—but don’t tell me one is better than the other. It’s not a question of one being better than the other, the question is what is needed for the condition of the person at any given time.
What you need to realize is each have their place, and what might work for one person in one case, might be different for another in another case. My assistant and I use both MMS1 and CDS and we have used CDH in the past. You can’t be rigid on this. And it is my opinion that you also can’t say use one “only if you don’t have the other”, like as a last resort. That is not very scientific. There might be a time and place for that, like if one is forced into it by circumstances. But overall what is the criteria? You don’t use one as a last resort, you use one or the other according to what the problem is, and according to the conditions of the body of the individual.
The question is, what does the body need? You have to look at all the variables and then decide. Stay open, listen to your body—it’s so important. If something is not getting any results, or showing any signs of improvement at all, even small signs within a reasonable amount of time, I would say try something else. I already wrote all about this in the Guidebook, (see below). And for Pete’s sake, follow the Three Golden Rules of MMS.
Another important point here is you gotta be practical about all the surrounding or existing conditions. For example, you have to look at the availability of things. Another factor on practicality and availability is also affordability of things. If someone can afford to purchase an expensive machine to make pure CDS, more power to you, but what about the millions of people in the world who do not have the means to do that? As I said when I stood on that street corner and declared “I’m going to take this to the world”. I meant ALL of mankind. Be careful about getting too complicated so that the common man can’t afford things. Again, give ‘em all the possibilities.
When I was in Africa, I taught ‘em how to measure the sodium chlorite solution without a scale—because out in the bush they didn’t have scales available. I taught how to test your solution using blue Gatorade if test strips were not available. I’m not knocking advancements, but you get my point? Don’t go shoving the simple ways under the carpet. And with the way the world is going, we might just have to get back to the basics like it or not.
If people do not learn the basics, it’s a detriment. It’s like building a house without a foundation. That is why I spent time writing the Guidebook. It is important to get the foundation, get the basics down and then branch out from there into variations and whatnot if you are so led and able. It’s great to experiment and learn and all of that, I’m all for it, but beware if you don’t have the basic principles down, and don’t go trying to bury one for the new.”
Following is taken from the MMS Health Recovery Handbook
Appendix A – CDS, CDH Basic Information
In this book I have chosen to not go into details on either CDS (Chlorine Dioxide Solution) or CDH (Chlorine Dioxide Holding). These are both variations of MMS1, each one requiring a different preparation, although all three are made from the same two ingredients; MMS and an acid activator.
The main goal of this book is to provide a solid foundation of the Health Recovery Plan using MMS1 and MMS2. Once you understand the principles in this book, you can apply them to CDS and CDH, both of which can be used with many MMS Protocols.
We are discovering new things about MMS all the time, and about CDS and CDH, which have been around for less time than MMS1. I taught about CDS in my previous book, as well as on instructional videos on YouTube, and about both CDS and CDH in seminars. Since that time, however, some of the information has changed. (So some former teaching and videos are now outdated.) It’s an ongoing process. Due to time and space, it is not possible to properly or thoroughly cover CDS and CDH in this book, and as mentioned above, it is important to understand the basic overall principles of MMS and the Health Recovery Plan first. Remember, as with MMS1, always use the Three Golden Rules of MMS (see pages 83-84) if you are using CDS or CDH.
With that said, here is some information regarding some of the differences between CDS, CDH and MMS1.
Over the years I have received a great deal of feedback both from Health Ministers around the world who are very active in helping others recover their health, and from individuals themselves, regarding the three forms of MMS (MMS1, CDS and CDH) and how they have worked for them.
I want to make it clear that we have seen all forms of MMS help people recover their health. Nevertheless, there are significant differences with each one. As MMS1 has already been covered extensively in this book, below is a brief synopsis of CDS and CDH.
CDS
CDS was developed by a cattle rancher with direct support and cooperation of Andreas Kalcker. (It was initially developed for use with animals.) CDS is chlorine dioxide gas in distilled water and contains no sodium chlorite or activator. It has to be made up ahead of time through one of several distillation processes and ideally stored in the refrigerator. A pre-made mixture can be convenient. Depending on how CDS is handled, it can last several weeks or even longer.
While CDS is relatively easy to make, there are many variables that can have an effect on the end product. Things such as temperature, climate, altitude, humidity, air pressure, and what type of equipment is used can make a big difference in the resulting CDS. For example, if there is too much air in the bottle or jar it is stored in, it can lose potency. Each time you open the bottle, out-gassing occurs which will lessen potency, and so on. Learning the techniques on how to make and handle CDS is not all that difficult if one is dedicated to doing so—but close attention must be given to the details.
CDS is fully activated—there is no residual sodium chlorite left in the solution—which is considered by some to be an advantage. It can be easier on the stomach, and many consider it to have little taste compared to MMS1. At low doses this is true. However, to recover health from serious disease, it is usually necessary to take high level doses of CDS. When this happens, taste and/or burning in the throat can enter into the equation, and sometimes a Herxheimer reaction.
CDS can be helpful for sensitive people, who for one reason or another cannot tolerate MMS1. We have seen that for some people starting out on CDS can be beneficial to help one become accustomed to taking MMS1. The Starting Procedure with MMS1 has eliminated the need for this in most cases. The above stated observations are regarding taking CDS internally. Some people feel that CDS works best with treating external conditions and many have had success with this.
The main important observation that myself and other extensive users of CDS (who have worked close with me) have noticed, is something which I call the plateau phenomena. Those working with autistic children used CDS exclusively for one year. At first it was easy to see the children were improving, but as time went on and the children continued to take CDS, the majority seemed to hit a plateau where they were not improving. They came to a standstill. But when these same children were put back on taking MMS1, they again started to improve.
Several Health Ministers and others, when using CDS for a variety of diseases, including cancer, have also reported this phenomenon. There seems to be a point when the individual hits a stalemate (this doesn’t always happen, but it often does), but when put on MMS1, they start to improve again. So, if you do use CDS, my advice would be to be aware of the plateau phenomena and if it happens to you, switch to MMS1.
A further word on CDS: There have been differences of opinion over the years regarding the dosing amounts of CDS and the equivalent of CDS to MMS1 for use in our protocols. In the past, we have published a ratio of 1 ml of CDS at 3000 ppm equals a 3-drop dose of MMS1. I have come to believe this is very low dosing for CDS. At the same time, I have come to realize, for multiple reasons too detailed to explain here, that an exact equivalent between CDS and MMS1 is not possible to determine.
This is in part due to the reasons mentioned above, the preparation and handling of CDS includes many variables. For example, you may start out with a 3000 ppm solution of CDS, but in a weeks’ time, due to out-gassing every time the bottle is opened and other factors, your solution may be getting increasingly weaker. Another reason exact equivalents are difficult to determine is due to the amount of a person’s stomach acid. Equivalents can perhaps be determined based on tests with simulated “normal” stomach acid. There are however, many things to consider, one being if the individual indeed does have “normal” stomach acid (most people who have poor health and who are in need of health recovery do not have normal stomach acid). As I have repeatedly said throughout this book, if one follows the Three Golden Rules of MMS, this will indicate if you need to increase or lower your dose.
Probably the most important reason we cannot equate amounts of MMS1 and CDS is that after passing through the stomach, MMS1 still has roughly 50% unactivated sodium chlorite which passes into the human system. Because sodium chlorite has been taken for more than 80 years by hundreds of thousands of people, many of whom swear by it, we must assume that the unactivated sodium chlorite must have some benefit to the system, in addition to the chlorine dioxide. (More on this below.) Since CDS has no sodium chlorite there is no way to make an evaluation of one against the other.
CDH
CDH was developed by Scott McRae and Charlotte Lackney. CDH is also “pre-made” and much easier to make than CDS. It also must be refrigerated. It lasts a couple of weeks to a month in the fridge, depending on the recipe used. CDH, like MMS1, is not totally activated, thus leaving some free sodium chlorite to continue on through the stomach into the system. I have not had extensive experience with CDH, therefore cannot say to use or not use it. We have received reports that it has produced good results for some users.
My Personal Conclusion on MMS1, CDS and CDH
As stated above, CDS is completely activated and contains no residual sodium chlorite in the solution. CDH and MMS1 do contain some free sodium chlorite which makes its way through the stomach into the system. Now, while some people believe the advantage to CDS is that it does not contain unactivated sodium chlorite, I have a different opinion. I believe just the opposite.
Unactivated sodium chlorite alone also destroys poisons and kills pathogens. It has been sold in health food stores in the USA for 80 years and many thousands of people have had some good results from taking it. There are those who now use it without prior activation because they believe that the stomach acid is what activates it and they get a certain amount of good results.
When I first discovered MMS, it was MMS (sodium chlorite) alone that healed the first men in the jungle of malaria. As I traveled throughout the jungle helping many more people recover their health (mostly from malaria and typhoid fever), it was sodium chlorite alone that helped. But the success rate was about 60%. Through much experimentation, it wasn’t until I developed the formula further and started activating MMS that the success rate for malaria turned out to be about 98%, and about 92-94% for other diseases.
It is my opinion, unactivated sodium chlorite penetrates deeper into the tissues of the body than even MMS1, according to data I have gleaned from patents issued in the last century. Unactivated sodium chlorite penetrates into the tissues in a different way than MMS1, and thus the two together seem to be more effective than either one alone. It has been very obvious to many of us that MMS1 (chlorine dioxide) along with unactivated sodium chlorite is what gets the very best results. This is anecdotal evidence, but with many thousands of people recovered, even scientists have to admit that serves as legitimate evidence.
In conclusion, I want to say that chlorine dioxide in all forms continues to be a mystery at times. The important thing is to find what works best for you. Remember to always use the Three Golden Rules of MMS (pages 83-84). If using CDS or CDH, and you are not seeing desired results, carefully study Chapter 8 in this book (MMS Health Recovery Guidebook) and/or consider switching to MMS1.
Is CDS pH neutral?
The following is from Dr. Martin Ramirez PhD (COMUSAV Engineer)
ATTENTION‼️
“To clarify the question, is CDS a neutral pH?
The answer is NO.
What is NEUTRAL is the ClO2 MOLECULE.
Once the gas enters the water its pH becomes acidic, this is why we almost always must dilute in water and is almost impossible to drink the concentrate.
“CDS is not a neutral solution, we have explained this in numerous occasions. People say “it’s neutral” and that is incorrect, it is a chemical solution. It is a neutral gas and when it comes in contact with water there is a reaction (slight one, but it does react) and it’s pH drops to acidic based on the type of water used.
Sometimes the pH drops to as low as 3.5 making it impossible to administer intravenously without irritating the person’s vein (in most cases). People may produce CDS at a neutral level, but after some time it will become acidic and that is a fact and has been measured.”
Source: Dr. Martin Ramirez, PhD (COMUSAV Engineer). (Inventor of the MARA CLO2 meter.)
Follow us in our official COMUSAV in English Channel:
https://t.me/OfficialChannelComusavUSA
https://t.me/OfficialChannelComusavUSA/425
The Importance of Testing CDS
Below is an article detailing the testing process and the results of various products. Click on the Up/Down arrows to move through the pages. You can also view the entire PDF directly in your browser by clicking HERE.


 Mix up a 3-drop dose of MMS1 to do this test, if you use less drops it will be difficult to adequately judge the color. It is best to carry out this test in a room with good lighting. When you have mixed your drops (before adding water), hold the glass up against a white or light colored background and look through the side and bottom of the glass (where your drops are) with the glass level with your eyes; at this angle you will be looking through your drop mixture. If you look down into the glass, the drops will often look lighter yellow, but if you view the drops at eye level (with good lighting) you should see a darker shade—that is, amber. Although it turns dark, it must also be transparent (see-through). The drops must appear amber in color. The amber color will fade and become light yellow in about 15 minutes. Do not let the solution sit for more than a minute before consuming it, as it will lose potency.
Mix up a 3-drop dose of MMS1 to do this test, if you use less drops it will be difficult to adequately judge the color. It is best to carry out this test in a room with good lighting. When you have mixed your drops (before adding water), hold the glass up against a white or light colored background and look through the side and bottom of the glass (where your drops are) with the glass level with your eyes; at this angle you will be looking through your drop mixture. If you look down into the glass, the drops will often look lighter yellow, but if you view the drops at eye level (with good lighting) you should see a darker shade—that is, amber. Although it turns dark, it must also be transparent (see-through). The drops must appear amber in color. The amber color will fade and become light yellow in about 15 minutes. Do not let the solution sit for more than a minute before consuming it, as it will lose potency.